

#13 PACE: A Comprehensive Care Model for Aging at Home
How a little-known Medicare program keeps nursing-home-eligible seniors at home, and why AgeTech should pay attention.

I’m always surprised at how many people, even those deeply engaged in healthcare and agetech, have never heard of PACE.
PACE stands for the Program of All-Inclusive Care for the Elderly. In many ways, it’s what healthcare should look like for older adults with chronic illnesses: preventative, coordinated, community-based, and centered around the whole person. The model traces back to 1971, when Dr. William Gee and social worker Marie-Louise Ansak founded On Lok (”peaceful, happy abode” in Cantonese) in San Francisco’s Chinatown to create a community-based alternative to nursing home care for immigrant elders.
I’ve spent the last several months getting closer to the PACE world through my work at Lightswitch Labs, where we are building tools to help aging services providers navigate technology. In doing so, I’ve spoken with PACE program leaders across the US. The more I learn, the more convinced I become that PACE represents a model worth understanding for broader agetech innovation.
Thank you to Jenn and Annie from MassPACE for their guidance and support for this article.
Why PACE is revolutionary
Most healthcare in the United States is reactive. You get sick, you see a doctor, you get a treatment, you get a bill. The system is organized around episodes of illness, not around keeping people well. For older adults with multiple chronic conditions -- and nearly 80% of older adults have two or more -- this fragmented approach is particularly harmful.
PACE flips this on its head.
A PACE program provides the entire continuum of care and services to older adults with chronic care needs: primary care, specialist visits, prescription drugs, physical and occupational therapy, adult day services, home care, meals, transportation, social work, and more. All of it is coordinated by an interdisciplinary team (IDT) that includes a primary care physician, nurse, social worker, physical therapist, dietitian, and other professionals who know the participant personally.
The emphasis is on prevention. Rather than waiting for a hospitalization or an ER visit, the team works to anticipate problems before they escalate. The PACE center, a physical facility where participants come for day services, socialization, and medical appointments, acts as a hub for this coordinated approach. Staff notice when someone is eating less, moving differently, or withdrawing socially. These early signals trigger intervention long before they become emergencies.
There’s another dimension of PACE that doesn’t get talked about enough: cultural awareness. PACE was born in San Francisco’s Chinatown, serving immigrant families from China, Italy, and the Philippines. That origin is not incidental: because PACE programs are rooted in specific communities and serve participants over long periods (the average enrollment is two to three years, and disenrollment is most commonly due to death), they develop a depth of cultural understanding that most healthcare settings simply cannot replicate. Programs can tailor meals, activities, language, and care practices to the communities they serve. This matters clinically: cultural competence improves trust, adherence, and outcomes, particularly among populations that have historically been underserved by the healthcare system.
The results are striking. Approximately 94% of PACE participants live in the community rather than in a nursing facility, even though every single one of them has been certified as needing a nursing home level of care.
How PACE Programs Are Structured
PACE operates under a unique financial and regulatory structure that sets it apart from virtually every other healthcare program in the country.
Eligibility
To enroll, an individual must be 55 years or older, live in the service area of a PACE program, and be certified by their state’s Medicaid agency as meeting the criteria for nursing home level of care. Enrollment is voluntary -- participants can disenroll at any time.
Medicaid eligibility isn’t required to enroll in PACE programs, but if one qualifies for Medicare but not Medicaid, the individual will pay a monthly premium out-of-pocket. This varies by state and can run up to a few thousand dollars a month. For this reason, most PACE participants are dually eligible.
Financing
Unlike fee-for-service healthcare, PACE uses a capitated payment model. Each PACE organization receives a fixed per-member-per-month (PMPM) payment from Medicare and Medicaid for each participant. For the roughly 84% of participants who are dually eligible for both Medicare and Medicaid, the organization receives capitated payments from both programs. Medicare payments are risk-adjusted based on participant demographics and diagnoses, similar to the model used for Medicare Advantage. Medicaid rates are set by each state, typically based on a discount to what the state would otherwise have paid for nursing home and community-based care for that population.
This capitation structure is critical: the PACE organization assumes full financial risk for all of a participant’s healthcare. If the organization keeps someone healthy and out of the hospital, it retains the savings. If a participant has a catastrophic health event, the organization absorbs the cost. There are no deductibles, copayments, or coinsurance for participants.
Startup costs
This is where starting a PACE program can become challenging. Before enrolling a single participant, an organization must secure a physical facility, outfit it as a day center and primary care clinic, hire and train the full IDT, navigate regulatory approvals from both the state and CMS, and build out operational infrastructure to manage full-risk capitation. This, along with working capital to cover initial operating losses, can run up to $5-$15M to start a PACE program.
HRSA has made up to $500,000 per year available through its Rural PACE Planning and Development grants, but for many prospective operators, the financial and operational lift remains daunting. This capital intensity is one of the key reasons PACE has been slow to scale despite its proven outcomes.
Business model implications
The PACE model creates fundamentally different incentives compared to fee-for-service or even most managed care. Because the organization bears full financial risk, it is incentivized to invest in prevention, care coordination, and social supports -- things that keep people healthy and independent. Transportation to the PACE center, a hot meal, and home safety assessments are not “nice to haves” but direct inputs to the financial model. Every avoided hospitalization and every deferred nursing home admission flows directly to the bottom line.
Where PACE Fits in Value-Based Care
If you follow healthcare policy, you’ve heard the term “value-based care” -- the idea that providers should be rewarded for keeping patients healthy rather than for the volume of services they deliver. The US healthcare system has been slowly transitioning toward value-based models for over a decade.
CMS has rolled out a spectrum of these arrangements. At one end, pay-for-performance programs add quality bonuses on top of fee-for-service. Then there are bundled payments, where a single payment covers an episode of care like a hip replacement. Shared savings programs like the Medicare Shared Savings Program organize providers into Accountable Care Organizations (ACOs) that share in savings and, increasingly, in losses. At the far end sits full-risk capitation: a fixed monthly payment per patient, with the provider bearing all cost risk.
What makes PACE distinct from other capitated models, including Medicare Advantage, is the scope and integration. Medicare Advantage plans are capitated, but they are insurance products that contract with networks of independent providers. PACE organizations don’t just pay for care; they directly provide it through their own IDTs and centers. And the capitation covers not just medical services but the full range of social supports, transportation, meals, home care, and long-term services. There is no other model in US healthcare that integrates medical, behavioral, and social care under a single capitated payment with full provider risk to this degree.
The Scale of PACE Today
For all its merits, PACE remains remarkably small.
As of the end of 2025, there were approximately 90,500 individuals enrolled in PACE across 198 programs in 33 states and the District of Columbia. To put that in context, there are over 60 million people enrolled in Medicare. Even among the subset of older adults who would qualify for PACE -- those certified as needing a nursing home level of care -- the program serves only a small fraction.
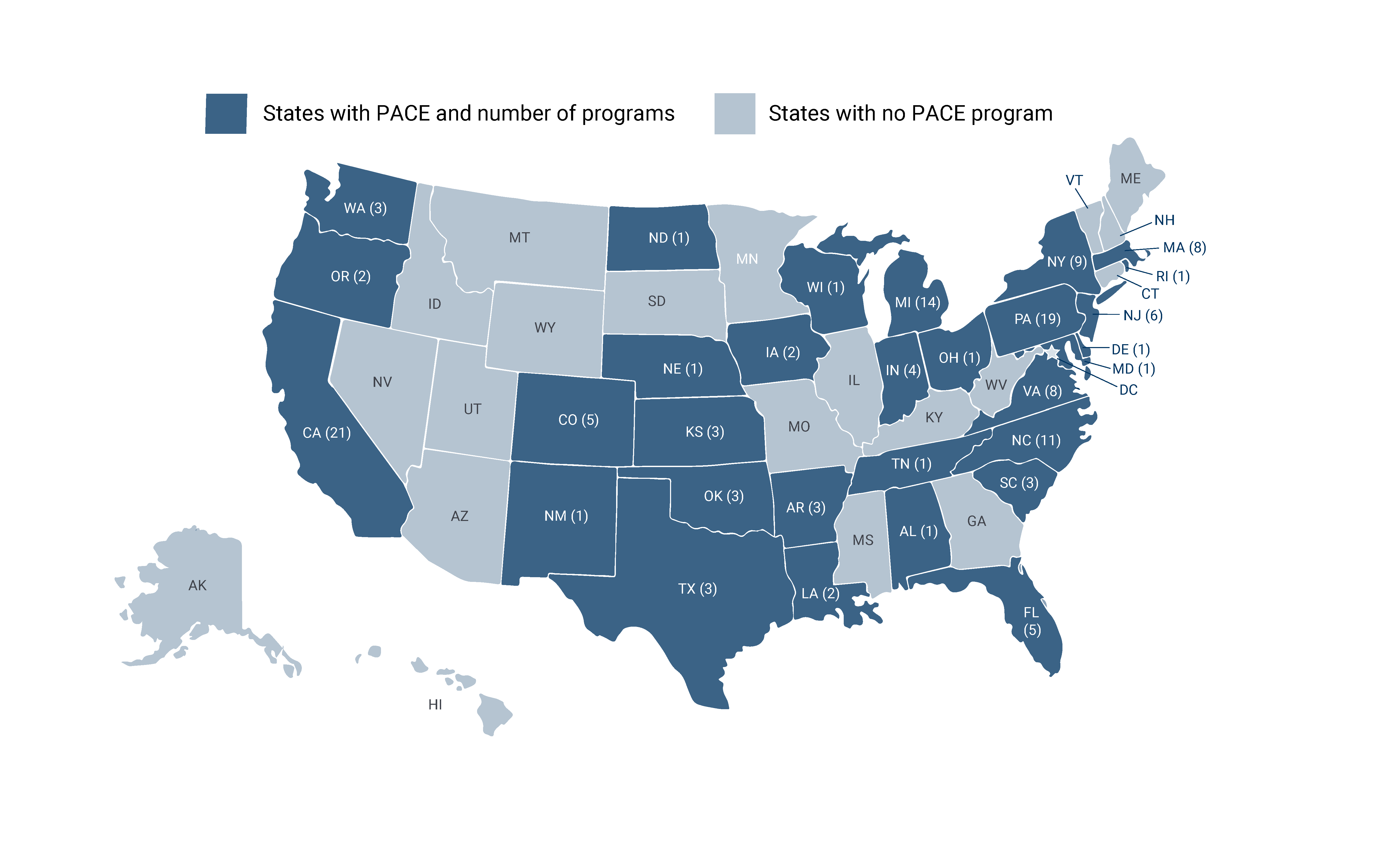
That said, PACE is growing. The last two years have been historic: 25 new programs opened in 2024, followed by 20 more in 2025. Prior to COVID-19, there were 130 programs in 30 states. Several states issued RFPs in 2025 to expand PACE into new markets, including New Jersey, Georgia, Oregon, Pennsylvania, Louisiana, and Tennessee. At the end of 2025, CMS announced a $50 billion initiative to strengthen healthcare in rural communities, which could further support PACE expansion.
Still, there are structural reasons why PACE has been slow to scale. As described above, the startup costs are significant. Beyond that, the service area for each program must be defined and approved, and states have different Medicaid rate-setting methodologies. In some cases the rates make it difficult for programs to sustain themselves financially.
Regulatory headwinds are also slowing PACE expansion. California, which has the largest concentration of PACE programs, is currently under a two-year application freeze: DHCS paused all new PACE applications and service area expansions in November 2025, citing the need to manage growth and maintain oversight capacity
The Future of PACE
Despite its modest footprint, there are reasons to believe PACE is entering a new phase of growth.
The demographic math is undeniable: over 10,000 Americans age into the older adult population every day. As this trend accelerates through 2050, demand for alternatives to nursing home care will only intensify, and PACE is one of the few proven models that delivers on this promise. Policy momentum is building alongside it. In January 2025 President Biden signed the Senator Elizabeth Dole 21st Century Veterans Healthcare and Benefits Improvement Act, giving veterans increased access to PACE across the country. More states are issuing RFPs for new programs, and NPA recently reached the milestone of 200 PACE programs nationally.
The PACE community is becoming better organized. State associations like MassPACE, CalPACE, and Florida PACE are growing in influence and actively working to improve the policy environment. The National PACE Association plays a critical role in federal advocacy. New programs are emerging in states that previously had none, and the Cherokee Nation recently launched the first tribal PACE program.
Private Capital and the PACE Growth Story
Perhaps the most telling signal of PACE’s momentum is the arrival of private capital. The economics explain the interest: each PACE member generates roughly $110K in capitated revenue per year from Medicare and Medicaid. A center with 200 enrollees -- the California average -- produces $22M in annual revenue, and that revenue is essentially guaranteed monthly from the government regardless of utilization. The model has fifty years of evidence, the unit economics are well-understood, and the addressable market is enormous relative to current enrollment.
A recent tracker identified roughly 30 PACE programs with private equity or venture capital backing as of 2025, up from just four in 2016. The new entrants are innovating in different ways. Seen Health raised a $22 million Series A led by 8VC to build a tech-native, culturally-focused PACE model -- starting with a center in LA’s San Gabriel Valley serving the Asian and Pacific Islander community, with a comprehensive operating system for care orchestration, providers who speak participants’ native languages, and care that incorporates Eastern medicine. Habitat Health, backed by $50 million from Kaiser Permanente, Town Hall Ventures, and NEA, is innovating on the go-to-market side: by partnering with an established health system like Kaiser, they can refer eligible members directly and accelerate the path from startup losses to a mature enrollment panel -- solving the j-curve problem that makes PACE so capital-intensive to launch. Their leadership team draws from Oak Street Health, Landmark Health, and Cigna/Evernorth, bringing deep value-based care operational expertise to PACE.
This influx of capital brings the potential for faster scaling, but it also raises some questions. The PESP report notes that PE firms in particular use debt to fuel growth, which can lead to cost-cutting in patient care and understaffing -- and that PE-backed firms accounted for 21% of all healthcare bankruptcies in 2024. For-profit PACE organizations are growing enrollment faster than nonprofits, but there is limited evidence on whether for-profit ownership affects care quality.
What Needs to Change for Growth to Be Sustainable
Growth momentum alone won’t be enough. For PACE to scale from 200 programs to 2,000, two foundational problems need to be addressed.
The evidence base needs to be strengthened. For all the enthusiasm within the PACE community, the program’s research foundation has real gaps. A scoping review from 2022 identified only six published studies directly comparing PACE outcomes to other caregiving programs. Policymakers and potential operators need robust, comparable data to justify the investment, and without it, PACE advocacy relies on testimonials and mission-driven enthusiasm -- which, while compelling, are not enough to move the needle with budget-conscious state legislatures.
The good news is that this gap is getting attention. In its June 2026 report to Congress, MACPAC recommended that CMS coordinate federal and state PACE audits, publicly release existing program-performance data, and develop a standardized national quality measure set — recommendations the National PACE Association applauded.
Programs must move from fragmentation to coordination.
PACE programs today are heterogeneous in their missions, organizational structures, and willingness to share data. In my conversations across multiple states, I’ve heard repeatedly that the community is close-knit but cautious. Programs operate with different electronic medical records, track different outcome measures, and are reluctant to share operational or quality data -- sometimes due to competitive dynamics, sometimes due to the politics of a small community. This fragmentation means that even within state associations, it is difficult to aggregate the kind of comparative data that would demonstrate PACE’s value at scale. The PACE community will need to build the data infrastructure and culture of transparency that enables shared learning, benchmarking, and credible advocacy. Individual programs operating as islands, however excellent, is not a scalable strategy.
PACE and Technology
If there is one theme that has emerged consistently from my conversations with PACE leaders, it is this: PACE programs want to adopt technology, but they face challenges in doing so.
To start off, the PACE model is uniquely well-positioned to benefit from technologies to support aging well. Because PACE programs are responsible for the full continuum of care and bear full financial risk, any technology that reduces hospitalizations, prevents falls, improves medication adherence, or enables more efficient care coordination has a direct and measurable impact on the program’s outcomes and finances. The IDT structure creates a natural integration point: the team already meets regularly to review participants, and technology that surfaces actionable data into that workflow can make a real difference.
So why isn’t adoption happening faster? From my conversations, three barriers stand out.
Budget. PACE programs operate under tight financial constraints, and technology spending often falls outside the core budget. In many cases, programs can only access new technology through grant funding, which means adoption is tied to grant cycles and application capacity rather than operational need. Smaller programs often lack the resources to even write the grant applications. And because existing outcome data is frequently outdated or inconsistent, it is difficult for program leaders to build a convincing ROI case for leadership. Without a clear financial case, technology investments feel discretionary, and they’re the first thing to get cut.
Capacity and implementation. Even when a program identifies a technology it wants to adopt, the challenge of actually implementing it is substantial. Many PACE programs lack dedicated IT staff. The people evaluating and deploying technology are the same clinicians and administrators already stretched thin by day-to-day care delivery. Staff burnout is real, and clinical teams are often resistant to changing workflows that, while inefficient, are at least familiar. One program leader told me that the biggest challenge isn’t finding the right vendor. The challenge is having anyone on staff with the time and expertise to manage the selection process, oversee implementation, train the team, and troubleshoot when things go wrong.
Patient population complexity. PACE serves one of the most complex patient populations in healthcare. Roughly half of PACE participants have dementia, and acuity levels vary dramatically across centers and over time. Many participants face cultural and language barriers. This means that technology deployed in a PACE setting must meet an exceptionally high bar: it needs to be simple enough for a participant with cognitive impairment, flexible enough to accommodate wide variation in functional ability, and useful to clinical staff without adding burden. A fall detection device that works well in independent living may be completely inappropriate for a PACE participant with advanced dementia. Any technology solution targeting PACE must be designed with this population’s specific needs in mind, and most are not.
These three barriers, budget, capacity, and population complexity, are interconnected and reinforcing. A program without IT staff can’t implement the tool even if funded, and a tool not designed for the population won’t deliver the outcomes needed to justify continued investment. Breaking this cycle will require not just better technology, but better infrastructure around technology adoption: consulting support for selection and implementation, grant-writing assistance, and resources that help programs navigate a landscape they don’t have time to figure out on their own.
Looking Ahead
PACE is one of those rare programs that actually works the way healthcare should. It is preventative, coordinated, person-centered, and community-based. It keeps older adults in their homes and aligns financial incentives with patient outcomes in a way that most of the healthcare system has struggled to achieve.
For AgeTech founders and investors, PACE represents a concentrated, underserved market of organizations that bear full financial risk for patient outcomes, which means they have both the motivation and the economic incentive to adopt technologies that work. The challenge is reaching them. As the PACE community grows, so does the opportunity to build the tools, data infrastructure, and platforms that help this model fulfill its promise.
I got a letter about this after crying in front of my mom's case manger, my mom's doctor, and the respite care woman who came in for 2-4 hrs, irregularly, once a week, and in 4 months only once helped my mom use the bathroom. By then she was in assisted living, because she couldn't manage in my house. I needed a stair lift and a new shower. After 2 wks, they put her on low dose opioids that helped her move around enough to manage, without sedating her too much. They never offered me those. They're paying $400/day. I didn't get a red cent.
There was a wonderful documentary highlighting On Lok by TalkingEyesMedia called Aging in America: The Years Ahead.